There are four biovars of C. diphtheria.
They are gravis, intermedius, mitis, and belfanti.
In diagnosis procedures it is not necessary to differentiate those into biovars.
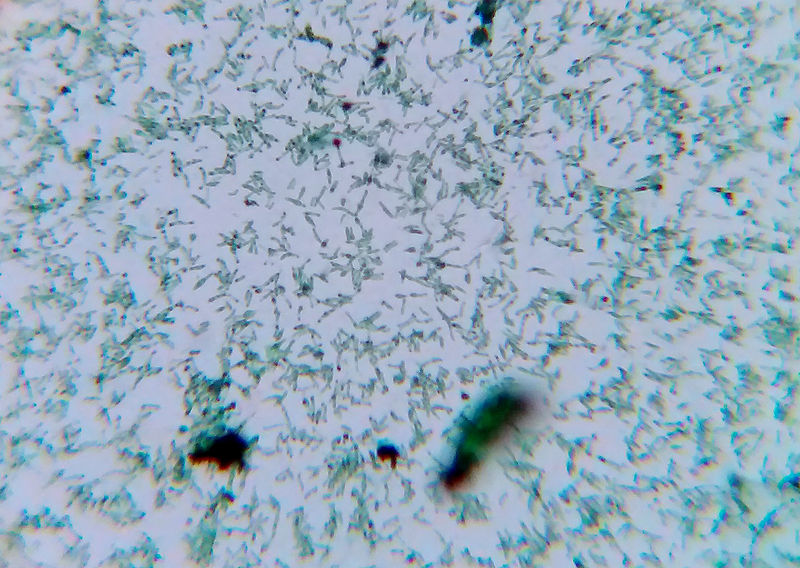
The major disease, diphtheria is caused by C. diphtheria.
It is an infection in tissues of upper respiratory tract (Nasal, nasopharyngeal and tonsillar diphtheria).
This specially occur in young children.
The infection is mainly caused by inhaling respiratory droplets.









No responses yet