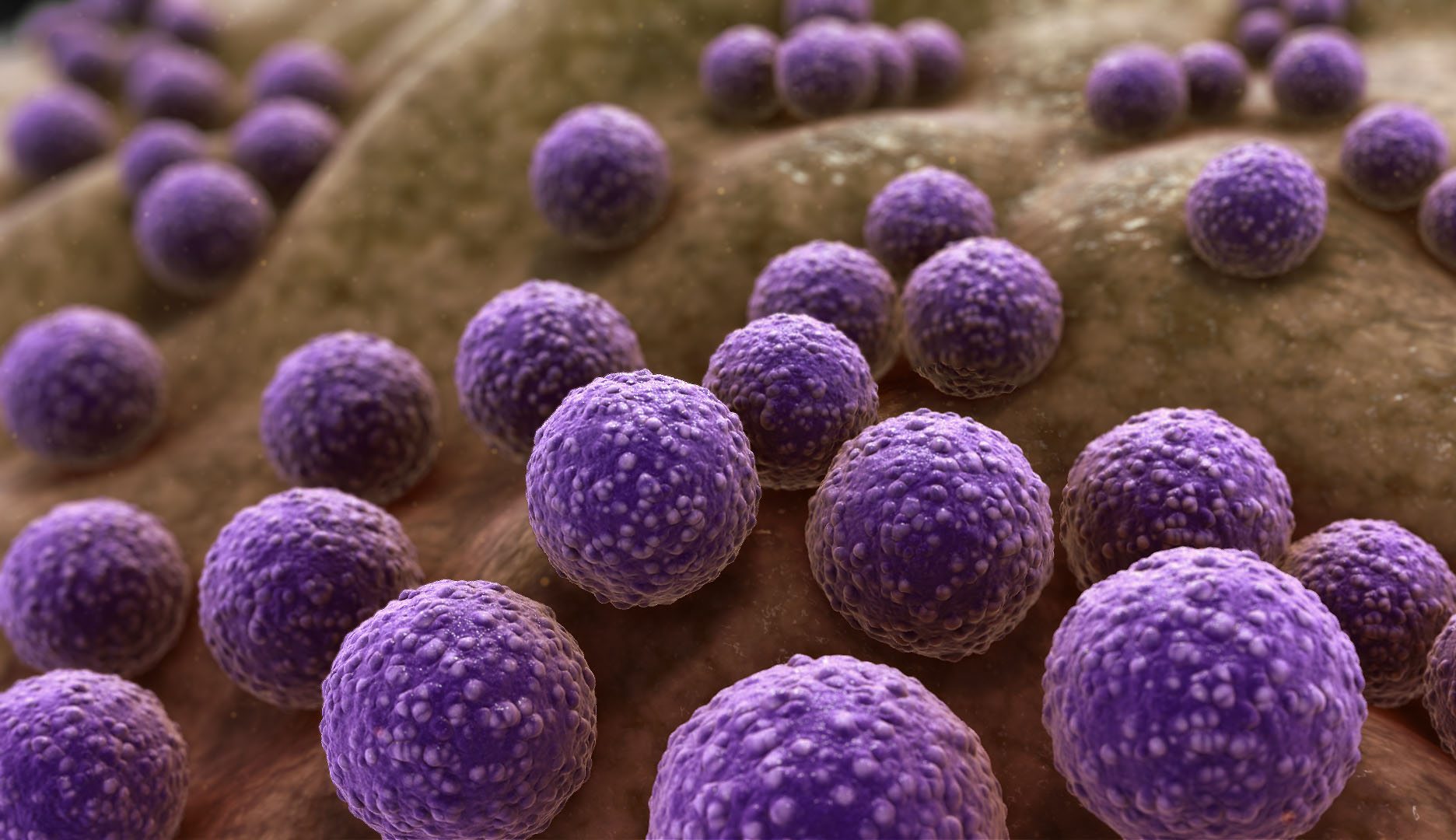
Now it uses as the genus name of facultatively anaerobic group. They may also can be found as part of the normal flora of other sites such as the upper respiratory tract, and are commonly present on animals. The major pathogen within the genus, S. aureus, causes a wide range of minor and major infections in human and animals. S. aureus causes suppuration, abscess formation, a variety of pyogenic infections and can even cause fatal septicemia. Pyogenic infections are Boils, Carbuncles, surgical site (wound) infection, abscesses (spinal), impetigo mastitis, blood stream infections, osteomyelitis, pneumonia (ventilator-associated) and Endocarditis. Toxin-mediated infections are Pemphigus neonatorum, toxic shock syndrome, Scalded skin syndrome and food poisoning.












No responses yet